Knee & Sports Injury Clinic
Bristol
Email: boc@orthopaedics.co.uk




Treatments
Browse through a rich range of information to find details of various treatments available for your condition. These include details on the treatment options, medications, physiotherapy and injections. Details are also provided on the range of surgical procedures and the rehabilitation following surgery.
You can also find out more about how to access private treatment when paying for yourself and the statutory quality criteria and success rates of our treatments.
Hover over links below to view summary or click on the link to view full article:
 Stinger Injury to the Shoulder and Neck in Rugby
Stinger Injury to the Shoulder and Neck in Rugby
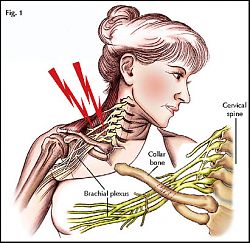
Collision in sport or in a road traffci accident can result in a sudden blow and depression of the shoulder joint. This can stretch the nerves which run from the cervicle spine to the arm through a confluence termed the Brachial Plexus. This can result in a temporary or more perminent damage to the nerves and a loss of fuction or sensation in the arm and hand. The sudden electric shouck or lightening bolt thoigh the shoulder gives the injury the term “Stinger” or “Burner Shoulder Injury”.
Burner and Stinger Injuries to the Shoulder
Burners and stingers are common injuries in contact or collision sports. A burner or a stinger is an injury to the nerve supply of the upper arm, either at the neck or shoulder. The injury is named for the stinging or burning pain that spreads from the shoulder to the hand. This can feel like an electric shock or lightning bolt down the arm.
Athletes who engage in contact sports are more likely to suffer a burner or stinger. Burners and stingers often occur with a fall onto the head, such as in Rugby, Judo, wrestling or a tackle or block in American football. The injury to the nerves which travel to the arm from the neck can be injured in the area of the brachial plexus. A sudden stretch of the brachial plexus nerves often happens when the head is forcefully pushed sideways and down in an impact or tackle. This bends the neck and pinches the surrounding nerves.
In most cases, burners and stingers are temporary and symptoms quickly go away. Burner and stinger symptoms typically occur in one arm only. They usually last seconds to minutes, but in 5% to 10 % of cases, they can last hours, days, or even longer.
Treatment of a Stinger injury begins by careful assessment of any more serious injury. In particular this must exclude an injury or fracture to the cervical spine. The patient need to have their cervical spine immobilised and to be removed from the field of play for medical assessment. Assessment of the patient will include an assessment of any residual nerve damage, neck or shoulder pain. Investigations may include X-rays or an MRI scan. Athletes are not allowed to return to sports activity until their symptoms are completely gone. This can take a few minutes or several days. Athletes should never be allowed to return to sports if they have weakness or neck pain.
Stinger’s should be differentiated from include fractures, dislocations, or damage to the ligaments (tissue connecting two bones) of the cervical spine. A spinal cord injury usually is associated with neck pain and causes residual and lasting nerve symptoms which are sometimes involving more than just one arm and possibly the legs. Such a more severe injury must be excluded by medial attendants and needs to be treated as a medical emergency.
If the attending and qualified team doctor or physiotherapist deems the injury minor with complete resolution of the symptoms, full pain free movement of the shoulder and cervical spine normal strength and feeling in the arm and hand then the athlete may be able to return to the game. It is much more common that patients need to be immobilised in a neck collar and seek medical attention and an X-ray or MRI scan.
Much more information on Spine and Shoulder injuries their diagnosis, investigation, treatment, physiotherapy and rehabilitation is available on
Shoulder Surgery: http://www.orthopaedicopiniononline.co.uk/index.php?id=24
Physiotherapy and Rehabilitation: http://www.orthopaedicopiniononline.co.uk/index.php?id=30
Author: DAVID P JOHNSON
MB ChB FRCS FRCS. MD
Consultant Orthopaedic Surgeon
www.Bristol-Knee-Clinic.co.uk
© OrthopaedicsOpinionOnline 2011 www.OrthopaedicOpinionOnline.co.uk
Disclaimer: The views expressed in this article are not necessarily those of Orthopaedic Opinion Online or the author. The information is provided for general background reading only and should not be relied upon for treatment. Advice should always be taken from a registered medical practitioner for individual circumstances and for treatment of any patient in any circumstances. No liability is accepted by Orthopaedic Opinion Online, or the author in respect to the information provided in respect of the content or omission or for any reason or as a result of treatment in individual circumstances. This information is not for use in the USA.